The removal of a tracheostomy tube is known as decannulation. Before decannulation can be considered, a child must be able to wear a cap over the tube while awake without experiencing airway distress. If the child can breathe adequately through their nose and mouth with the tracheostomy tube covered, the tube is capped overnight in an ICU, where heart rate, respiratory rate, and oxygen levels are closely monitored. If the child experiences no difficulties, the tracheostomy tube is removed the next day.
| Characteristics | Values |
|---|---|
| When to take off tracheostomy tube | When a child is able to wear the cap for all waking hours without any airway distress or difficulties, and is growing and gaining weight |
| Process | Decannulation is a two- to three-day process done in the pediatric intensive care unit in the hospital |
| First night | The tracheostomy tube is kept capped while the child sleeps. Heart rate, respiratory rate, and oxygen levels are closely monitored |
| Second night | If the child has no difficulties with the overnight capping trial, then the tracheostomy tube is removed the following day by the ENT team |
| Conditions | Before decannulation, a tonsillectomy and/or adenoidectomy may be recommended to prevent airway obstruction during sleep |
| Aftercare | The TC fistula should be kept covered with a small bandage until it is fully closed to protect the child's airway from foreign objects or particles in the air |
Explore related products






What You'll Learn
- Capping during sleep should be done under ICU observation or during a sleep study
- Decannulation can be considered when a child can wear a cap during waking hours without airway distress
- A tonsillectomy may be recommended before decannulation to prevent airway obstruction during sleep
- The TC fistula should be covered with a bandage to protect the child's airway
- A microlaryngoscopy and bronchoscopy must be done to ensure the child's entire airway is open
![]()
Capping during sleep should be done under ICU observation or during a sleep study
Capping the tracheostomy tube during sleep should be done under ICU observation or during a sleep study, and only in patients who have tolerated capping during wakefulness. The patient is initially monitored with the tracheostomy tube uncapped. Then, the tube is capped, and airflow and end-tidal PCO2 are monitored via the nose and mouth. If there is concern that the patient may not tolerate the procedure, it can be done as a bedside study in the intensive care unit.
Sleep studies are typically performed at a sleep center or hospital, where a technologist places electrodes on the patient to record body functions and sleep variables. Cameras may also record the patient's movements during sleep. Sleep studies can also be performed at home, where a monitoring device records sleep data, often for several nights. Sleep studies help diagnose sleep-related disorders and determine what affects a person's sleep. They evaluate a person's typical sleep quality and are generally full-night procedures.
Preparing for a sleep study involves following provider guidelines on bathing and grooming. It is recommended to bathe or shower beforehand, but avoid using creams, lotions, or hair care products afterward, as these can interfere with sensor readings. Alcohol and caffeine consumption should also be minimized on the day of the study, as they can affect sleep.
Sleep studies require electrodes to be placed on the patient's body, so it is important to avoid using any skin or hair products that could interfere with the adhesion of the electrodes. This includes makeup, gels, and lotions. Nail polish and fake nails should also be avoided, as they can affect pulse oximeter readings.
Sleeping Pills: What's Inside?
You may want to see also
Explore related products



![Vakly Split Drain Sponge Gauze 4x4 Sterile 6 Ply Pads [Pack of 50] Absorbent Precut 4"X4" Non-Woven Slit Bandage for I.V. Tracheostomy - 25 Packs of 2 Pre Cut Bandages + 1 Roll of Medical Tape](https://m.media-amazon.com/images/I/715njgPrkGL._AC_UL320_.jpg)

![]()
Decannulation can be considered when a child can wear a cap during waking hours without airway distress
Decannulation is the removal of a tracheostomy tube. This procedure is considered when the initial medical conditions that required a child to have a tracheostomy have been resolved. Before decannulation, a child must be able to breathe effectively without the tracheostomy tube, and their lungs must be healthy enough.
Capping is an important step in the decannulation process. During capping, the tracheostomy tube is blocked, and the child breathes through their nose and mouth. The child must be able to tolerate capping for all waking hours without any signs of airway distress or difficulties. This is because the child's tracheostomy tube should always remain uncapped while they sleep, as signs of airway distress may be too subtle for family members or nurses to recognize, which can lead to cardiac arrest.
The first capping trial is done in the presence of a surgeon, who closely monitors the child's tolerance to breathing through their nose and mouth. The amount of time the child wears the cap is then gradually increased. If the child can tolerate capping all day, they will be admitted to the hospital for a capped sleep study to observe their breathing during sleep. If the sleep study is normal, the tracheostomy tube is removed during the same admission.
After decannulation, the child will follow up with their airway surgeon around four to six weeks later. Sometimes, the tracheostomy stoma site closes by itself, but other times, additional surgery is needed to close the stoma.
Mixing Xanax and Herbal Sleeping Pills: A Safe Combination?
You may want to see also
Explore related products






![]()
A tonsillectomy may be recommended before decannulation to prevent airway obstruction during sleep
Decannulation is a two- to three-day process that is carried out in a pediatric intensive care unit in the hospital. Before this process, a child with a tracheostomy will sometimes have large tonsils and/or adenoids, which can cause airway obstruction during sleep after the tracheostomy tube is removed. To prevent this, an ENT surgeon may recommend a tonsillectomy and/or adenoidectomy before decannulation. Tonsillectomy is the surgical removal of the tonsils, which are round, fleshy masses in the back of the throat.
Tonsillectomies are recommended for two main reasons: to treat breathing-related sleep disorders such as sleep apnea and to reduce the risk of infection in people with frequent or chronic tonsillitis. The procedure helps almost all normal-weight children with sleep-disordered breathing (SDB) and improves sleep in most children in this group. Tonsillectomy also helps overweight children with SDB, but sleep is not always improved.
Tonsillectomies are usually outpatient procedures, meaning the patient can go home on the same day. However, if complications arise, the patient may be kept in the hospital overnight for monitoring. Tonsillectomy recovery takes up to two weeks, during which the patient can expect throat pain and other side effects, such as swelling of the tongue or roof of the mouth.
Before a tonsillectomy, a healthcare provider will perform a routine check and may request blood tests to ensure the patient is healthy enough for surgery. During the procedure, the patient is kept asleep and comfortable with general anesthesia. After the surgery, the patient will need to follow detailed preoperative instructions provided by their healthcare provider to ensure a smooth recovery.
Sleeper Agents: America's Covert Operations?
You may want to see also
Explore related products






![]()
The TC fistula should be covered with a bandage to protect the child's airway
A tracheostomy is a surgical procedure that creates an opening in the neck, allowing direct access to the trachea (windpipe). This opening, known as a tracheostomy tube or stoma, provides an alternative airway for individuals who have difficulty breathing through their nose or mouth. This procedure is often performed on children with respiratory issues to facilitate breathing.
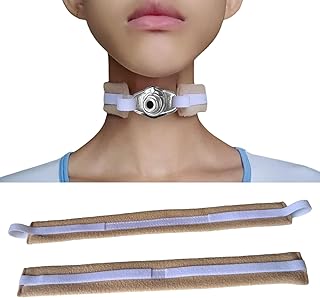
The TC fistula, or tracheocutaneous fistula, is the site where the tracheostomy tube is inserted, creating a direct connection between the trachea and the outside environment. It is crucial to keep this area clean and protected, especially when the child is sleeping. Covering the TC fistula with a bandage serves as a protective barrier, safeguarding the child's airway and preventing potential complications.
By covering the TC fistula with a bandage, foreign objects and irritants are prevented from entering the tracheostomy tube. Children may be curious and inadvertently touch or pull at the tube, so a bandage acts as a physical barrier, deterring them from tampering with it. Additionally, the bandage helps to secure the tube in place, reducing the risk of accidental dislodgement during sleep.
Moreover, the bandage aids in maintaining a clean and sterile environment around the tracheostomy site. It absorbs any secretions or mucus that may accumulate, reducing the risk of infection and ensuring the child's airway remains unobstructed. The bandage also provides a layer of protection against external contaminants, such as dust, pet hair, and mould spores, which could otherwise enter the tracheostomy tube and cause irritation or respiratory issues.
In the event of an emergency, the bandage can be quickly and easily removed to access the tracheostomy tube. It serves as a visual indicator of the tracheostomy site, enabling caregivers to act swiftly and efficiently if any issues arise during sleep. Additionally, the bandage can be inspected regularly to ensure it remains clean and intact, providing an extra layer of safety and peace of mind.
In conclusion, covering the TC fistula with a bandage is a crucial step in protecting a child's airway during sleep. It safeguards against potential obstructions, irritants, and infections, while also securing the tracheostomy tube in place. This simple measure significantly contributes to the overall safety and well-being of a child with a tracheostomy.
Melatonin Alternatives: Natural Sleep Aids for Restful Slumber
You may want to see also
Explore related products






![]()
A microlaryngoscopy and bronchoscopy must be done to ensure the child's entire airway is open
A microlaryngoscopy and bronchoscopy are procedures that allow doctors to examine a child's airway and address any obstructions or issues. The procedures are often performed to ensure the child's airway is open and unobstructed, especially after they have had a tracheostomy.
Microlaryngoscopy involves the use of a laryngoscope, a special telescope, or an operating microscope to get a magnified view of the larynx (voice box) and the surrounding airway. This procedure is particularly useful for evaluating and treating conditions affecting the vocal cords, such as hoarseness, breathing abnormalities, and speech abnormalities. During the procedure, surgeons can also remove polyps, masses, or foreign objects from the airway using special tools and techniques, including the use of a CO2 laser.
Bronchoscopy, on the other hand, involves the insertion of a long, flexible tube called a bronchoscope through the nose or mouth into the lungs. The bronchoscope has a small camera that allows doctors to visualize the vocal cords, trachea, and airways in the lungs. This procedure helps doctors identify blockages, narrowing, abnormal secretions, or foreign objects in the airway. It is also used to evaluate wheezing, chronic cough, and other respiratory issues.
When performed together, microlaryngoscopy and bronchoscopy provide a comprehensive evaluation of the child's entire airway, from the nasopharynx down to the lungs. This ensures that any obstructions or issues are identified and addressed, improving the child's breathing and overall respiratory health.
The procedures are generally safe when performed by experienced surgeons, but there are some risks and complications to consider. These include irritation to the airway and vocal cords, bleeding, temporary breathing problems, and heart rhythm issues. However, with proper care and monitoring, these complications are typically manageable.
Sleeping Pills and Abilify: Safe Mix?
You may want to see also
Frequently asked questions
Taking the trach off while sleeping, or decannulation, is done to evaluate whether a patient can breathe without the tracheostomy tube. This is done in a controlled setting with medical supervision.
A patient who can wear a cap on the tracheostomy tube during waking hours without airway distress and is growing and gaining weight is a good candidate for decannulation.
During the first night, the tracheostomy tube is capped while the patient sleeps. Parameters such as heart rate, respiratory rate, and oxygen levels are closely monitored. If the patient does not face any difficulties, the tracheostomy tube is removed the next day.