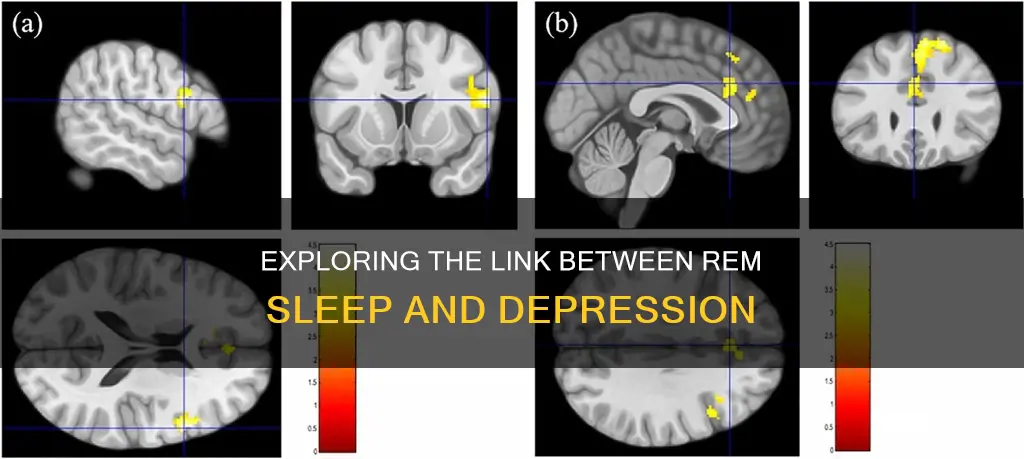
Sleep disturbances are a common symptom of depression, with up to 90% of depressed individuals reporting disrupted sleep. Polysomnographic sleep research has shown that depression is associated with altered sleep architecture, including a decrease in slow-wave sleep (SWS) production and disturbed rapid eye movement (REM) sleep regulation. Shortened REM latency, increased REM sleep duration, and increased REM density have been considered biological markers of depression, which can be used to predict relapse and recurrence.
REM sleep dysregulation in depression has been linked to a genetic predisposition to develop the illness, and it is also believed that REM sleep disinhibition may be part of a maladaptive stress reaction with increased allostatic load. Furthermore, REM sleep alterations may contribute to the development of central symptoms of depression, such as negative self-esteem and the overnight consolidation of negative emotional memories.
The relationship between REM sleep and depression is further supported by the fact that almost all antidepressants, which have varying mechanisms of action, selectively suppress REM sleep as an unintended side effect. Additionally, studies have shown that acute sleep deprivation can paradoxically improve depressive symptoms, indicating a complex bidirectional relationship between sleep and depression.
| Characteristics | Values |
|---|---|
| REM sleep | Altered sleep architecture |
| Decreased slow wave sleep (SWS) production | |
| Shortened REM latency | |
| Increased REM sleep duration | |
| Increased REM density | |
| REM sleep alterations may precede the clinical expression of depression | |
| REM sleep alterations may be useful in identifying subjects at high risk for the illness | |
| REM sleep changes may contribute to the development of central symptoms of depression | |
| REM sleep dysregulation in depression may be linked to a genetic predisposition/vulnerability to develop the illness | |
| REM sleep disinhibition may be part of a maladaptive stress reaction with increased allostatic load | |
| Antidepressants | Most antidepressants suppress REM sleep |
| Withdrawal of REM-suppressing antidepressants is followed by REM rebound |
Explore related products






What You'll Learn
- REM sleep dysregulation as a biological marker for depression
- REM sleep abnormalities as a predictor of depression relapse
- Antidepressants' suppression of REM sleep
- The cholinergic-aminergic imbalance model of REM sleep abnormalities in depression
- The role of stress in the link between REM sleep and depression
![]()
REM sleep dysregulation as a biological marker for depression
Sleep disturbances are typical for most depressed patients and are considered core symptoms of the disorder. Since the 1960s, sleep research has shown that depression is associated with altered sleep architecture, including a decrease in slow-wave sleep (SWS) production and disturbed rapid eye movement (REM) sleep regulation.
Shortened REM latency, increased REM sleep duration, and increased REM density have been considered biological markers of depression, which might predict relapse and recurrence. These REM sleep alterations may even precede the clinical expression of depression and could, therefore, be useful in identifying people at high risk for the illness.
REM sleep dysregulation in depression may be linked to a genetic predisposition/vulnerability to develop the illness. It is also conceivable that REM sleep disinhibition is part of a maladaptive stress reaction with increased allostatic load.
The disturbances of norepinephrine and serotonin systems may contribute to REM sleep abnormalities in depression. Antidepressants that increase the level of norepinephrine and serotonin or the affinity of their receptors in synapses are found to influence REM sleep strongly.
Delta Waves: The Link to REM Sleep Explained
You may want to see also
Explore related products



![]()
REM sleep abnormalities as a predictor of depression relapse
Sleep disturbances are typical for most depressed patients and are considered core symptoms of the disorder. Since the 1960s, research has shown that depression is associated with altered sleep architecture, including a decrease in slow-wave sleep (SWS) production and disturbed rapid eye movement (REM) sleep regulation. Shortened REM latency, increased REM sleep duration, and increased REM density have been identified as biological markers of depression, indicating a potential relapse or recurrence.
High-risk studies, including healthy relatives of patients with depression, suggest that REM sleep alterations may precede the onset of clinical depression. These alterations may be useful in identifying individuals at high risk for developing the illness. Several models have been developed to explain REM sleep abnormalities in depression, such as the cholinergic-aminergic imbalance model and chronobiologically inspired theories. Furthermore, REM sleep alterations are now considered not just as biological "scars" but as true endophenotypes of depression.
The complex relationship between REM sleep and depression involves genetic, neurochemical, and neurobiological factors. One hypothesis suggests that REM sleep dysregulation in depression may be linked to a genetic predisposition or vulnerability to developing the illness. Additionally, REM sleep disinhibition may be a part of a maladaptive stress reaction with increased allostatic load.
Further research is needed to fully understand the role of REM sleep changes in the development of central symptoms of depression, such as cognitive distortions, negative self-esteem, and the overnight consolidation of negatively toned emotional memories.
Effective Treatments for REM Sleep Disorder
You may want to see also
Explore related products






![]()
Antidepressants' suppression of REM sleep
Sleep disturbances are a core symptom of depression, with up to 90% of depressed individuals reporting disrupted sleep. Antidepressants, therefore, aim to normalise sleep. However, many antidepressants with activating effects, such as fluoxetine and venlafaxine, may disrupt sleep in the short term, while those with sedative properties, such as doxepin, mirtazapine and trazodone, can rapidly improve sleep.
The impact of antidepressants on sleep depends on the type of drug, dose, time of administration and duration of treatment. For instance, selective serotonin reuptake inhibitors (SSRIs) and tricyclic antidepressants (TCAs) have differing effects on REM sleep. While most antidepressants suppress REM sleep, SSRIs such as paroxetine and citalopram inhibit REM sleep without a subsequent homeostatic response to recover the lost REM sleep. Conversely, the TCA imipramine elicits a homeostatic response similar to that of REM sleep restriction, indicating that the REM sleep homeostat remains active even in the presence of pharmacological REM sleep inhibition.
Antidepressants with antihistaminergic action or strong antagonistic action at serotonergic receptors often improve sleep quality. For example, low doses of doxepin are prescribed for primary insomnia and have been shown to alleviate insomnia symptoms. Mirtazapine has also been associated with improved sleep quality after the first dose. However, it is important to note that mirtazapine can cause weight gain and induce nightmares.
While trazodone can improve sleep continuity and has minimal effects on REM sleep, it often results in daytime somnolence. Nefazodone, which has a similar mechanism to trazodone, has been shown to preserve sleep continuity and avoid REM suppression. However, reports of liver toxicity have limited its use in recent years.
Bupropion is another antidepressant that does not suppress REM sleep. Instead, it increases REM sleep time and may cause insomnia in some cases.
In summary, while most antidepressants suppress REM sleep, certain drugs, such as trazodone, nefazodone and bupropion, have minimal effects on or can even increase REM sleep. The choice of antidepressant depends on various factors, including the desired effects on sleep.
Sleep Apps: Detecting REM Sleep, How Does It Work?
You may want to see also
Explore related products






![]()
The cholinergic-aminergic imbalance model of REM sleep abnormalities in depression
Sleep disturbances are typical for most depressed patients and are considered core symptoms of the disorder. Polysomnographic sleep research has demonstrated that depression is associated with altered sleep architecture, including a decrease in slow-wave sleep (SWS) production and disturbed rapid eye movement (REM) sleep regulation. Shortened REM latency, increased REM sleep duration, and increased REM density have been considered biological markers of depression.
Several models have been developed to explain REM sleep abnormalities in depression, including the cholinergic-aminergic imbalance model. This model is based on findings from animal experiments that show the regulation of REM and non-REM sleep is governed by cholinergic and serotonergic/adrenergic neurons in the brain stem. Cholinergic neurons in the gigantocellular field of the tegmentum appear to trigger and maintain REM sleep.
Further evidence for the cholinergic-aminergic imbalance model comes from research showing that cholinomimetics can induce depression-like symptoms such as anhedonia and anergia in healthy volunteers. Additionally, depressed patients exhibit supersensitive responses to cholinergic challenges, including increased anergia and anhedonia, heightened cortisol levels, and dramatically shortened REM sleep latency.
Overall, the cholinergic-aminergic imbalance model of REM sleep abnormalities in depression suggests that imbalances in cholinergic and aminergic neurotransmission contribute to the sleep disturbances often observed in depressed individuals.
Actigraphy: Measuring REM Sleep Accurately?
You may want to see also
Explore related products






![]()
The role of stress in the link between REM sleep and depression
Sleep disturbances are a core symptom of depression, with up to 90% of depressed individuals reporting sleep problems. Research has shown that depression is associated with altered sleep architecture, specifically a decrease in slow-wave sleep (SWS) production and disturbed rapid eye movement (REM) sleep regulation. These REM sleep alterations, such as shortened REM latency, increased REM sleep duration, and increased REM density, are considered biological markers of depression and can even precede the onset of clinical depression.
Stress plays a significant role in the link between REM sleep and depression. While the relationship is complex and bidirectional, it is suggested that insufficient sleep can lead to stress, which in turn contributes to the development of psychiatric disorders like depression. This accumulation of stress can result from the deterioration of mental health due to sleep disturbances. Additionally, REM sleep disinhibition is hypothesized to be part of a maladaptive stress reaction with an increased allostatic load, contributing to the development of central symptoms of depression.
The impact of stress on REM sleep and depression is further supported by animal studies. These studies have shown that stress-related mood disorders have a significant impact on healthcare systems, and understanding the role of stress is crucial for developing effective treatments. Furthermore, animal models of depression are expected to aid in identifying the neuronal circuits that connect stress, sleep, and depression.
While the exact mechanisms are still being explored, the link between REM sleep and depression, with stress playing a pivotal role, is well-established. Further research and understanding of this complex relationship will help develop strategies to prevent and treat depression effectively, targeting sleep and stress management.
The Importance of REM Sleep and How Much We Need
You may want to see also
Frequently asked questions
REM sleep is a component of the sleep cycle characterised by random eye movements, reduced muscle tone, and an increased heart rate. It is associated with memory consolidation and generally makes up 20% of total sleep per night.
There is a well-known but not well-understood relationship between REM sleep and depression. Sleep disturbances are commonly reported in depressed individuals. Evidence provided by polysomnography shows that dysregulation of REM sleep is common in individuals with depression. A shortened REM latency, increased REM density, and increased total REM duration are regarded as biological markers of depression. REM sleep dysregulation is also a predictor of prognosis and can be used to predict the relapse and recurrence of depression.
There are several models that attempt to explain the link between REM sleep and depression. The two-process model, for example, describes how sleep-wake regulation is controlled by two processes: process S, which refers to the homeostatic process, and process C, which refers to the circadian control of the sleep-wake cycle. According to this model, depressed patients experience insufficient process S, which leads to their symptoms through disinhibition of REM sleep. The cholinergic-aminergic imbalance theory, on the other hand, suggests that depression is caused by the depletion of serotonin, dopamine, and noradrenaline in the central nervous system, coupled with the hyperactivity of acetylcholine neurotransmission.