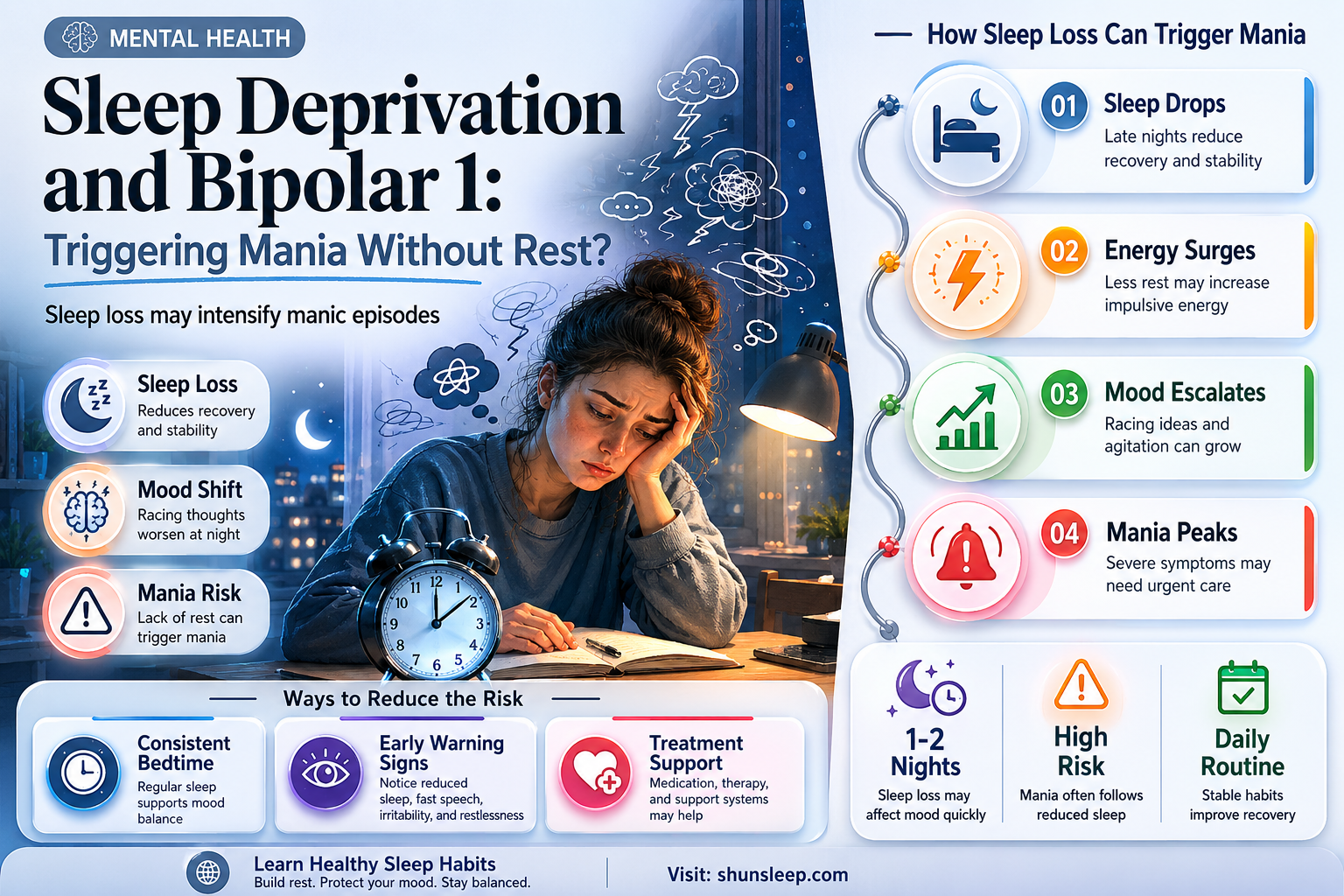
Bipolar I disorder is characterized by episodes of mania and depression, with mania being a defining feature marked by elevated mood, increased energy, and reduced need for sleep. One critical question often arises: Can a lack of sleep trigger manic episodes in individuals with Bipolar I? Research suggests that sleep deprivation, particularly in vulnerable individuals, can indeed act as a potent trigger for mania. Sleep disturbances disrupt the delicate balance of neurotransmitters and circadian rhythms, which are already dysregulated in bipolar disorder. Even a single night of insufficient sleep or irregular sleep patterns can destabilize mood, potentially leading to a full-blown manic episode. This highlights the importance of maintaining consistent sleep hygiene as a crucial component of managing Bipolar I disorder and preventing mood destabilization.
| Characteristics | Values |
|---|---|
| Sleep Deprivation as a Trigger | Yes, sleep deprivation is a well-documented trigger for manic episodes in Bipolar 1 Disorder. |
| Mechanism | Sleep loss disrupts circadian rhythms and neurotransmitter balance, leading to increased dopamine and norepinephrine activity, which can precipitate mania. |
| Prevalence | Approximately 25-30% of individuals with Bipolar 1 Disorder report sleep deprivation as a direct trigger for manic episodes. |
| Duration of Sleep Loss | Even one night of significantly reduced sleep (less than 4 hours) can increase the risk of mania in susceptible individuals. |
| Individual Variability | Sensitivity to sleep deprivation varies; some individuals may experience mania after minimal sleep loss, while others may require more prolonged deprivation. |
| Preventive Measures | Maintaining a consistent sleep schedule, practicing good sleep hygiene, and addressing sleep disorders are critical in managing Bipolar 1 Disorder. |
| Clinical Implications | Clinicians often emphasize the importance of sleep regulation as part of a comprehensive treatment plan for Bipolar 1 Disorder. |
| Research Support | Numerous studies, including those from the Journal of Affective Disorders and Biological Psychiatry, support the link between sleep deprivation and mania in Bipolar 1 Disorder. |
| Dual Relationship | Mania can also cause sleep disturbances, creating a bidirectional relationship between sleep and mood episodes. |
| Treatment Considerations | Medications and therapies that stabilize sleep patterns, such as mood stabilizers and cognitive-behavioral therapy for insomnia (CBT-I), are often recommended. |
Explore related products






What You'll Learn
![]()
Sleep Deprivation Triggers
Sleep deprivation is a well-documented trigger for manic episodes in individuals with Bipolar 1 Disorder. Research consistently shows that even a single night of insufficient sleep can disrupt the delicate balance of brain chemicals and neural circuits, potentially leading to mood destabilization. For those with Bipolar 1, this disruption often manifests as the onset of mania or hypomania. The relationship between sleep and mood is bidirectional; while mania can cause insomnia, lack of sleep can also precipitate manic symptoms, creating a dangerous cycle. Understanding this trigger is crucial for managing the disorder effectively.
One of the primary mechanisms linking sleep deprivation to mania involves the dysregulation of neurotransmitters such as dopamine and norepinephrine. Sleep loss increases dopamine activity in the brain, which is associated with heightened arousal, euphoria, and increased goal-directed behavior—hallmarks of manic episodes. Additionally, sleep deprivation affects the amygdala and prefrontal cortex, regions of the brain responsible for emotional regulation and decision-making. When these areas are impaired, individuals become more susceptible to impulsive behaviors and exaggerated mood elevations characteristic of mania.
Another critical factor is the disruption of the body’s circadian rhythm, which plays a significant role in mood regulation. For people with Bipolar 1, even minor shifts in sleep patterns can destabilize their circadian rhythm, triggering manic symptoms. This is why irregular sleep schedules, late nights, or pulling all-nighters are particularly risky. The body’s internal clock is closely tied to mood stability, and any interference can have profound consequences for those predisposed to mania.
Behavioral and environmental factors also contribute to sleep deprivation as a trigger. Stress, overstimulation, and excessive activity can lead to difficulty falling or staying asleep, especially during manic episodes. However, even in euthymic (stable) states, poor sleep hygiene, such as excessive screen time before bed or an inconsistent sleep routine, can increase vulnerability to mania. Addressing these factors through structured sleep habits and stress management is essential for preventing sleep-related mood episodes.
Finally, it’s important to recognize that sleep deprivation does not affect everyone with Bipolar 1 in the same way. Individual sensitivity to sleep loss varies, and some may experience mania after only a few hours of missed sleep, while others may require more significant deprivation. Monitoring sleep patterns and identifying personal thresholds are key components of a proactive management plan. Collaborating with healthcare providers to develop strategies for maintaining consistent sleep can significantly reduce the risk of mania triggered by sleep deprivation.
Why Does My Tongue Feel Dry After Sleeping? Causes & Solutions
You may want to see also
Explore related products






![]()
Mania Onset Mechanisms
Sleep deprivation has a profound and complex relationship with mania onset in individuals diagnosed with Bipolar I Disorder (BD-I). While not all individuals with BD-I will experience mania solely due to lack of sleep, sleep disruption is a well-established trigger for manic episodes. Understanding the mechanisms behind this phenomenon is crucial for both prevention and management.
Neurotransmitter Imbalance: Sleep deprivation disrupts the delicate balance of neurotransmitters in the brain, particularly dopamine and norepinephrine. These neurotransmitters play a key role in regulating mood, energy, and arousal. In individuals with BD-I, who may already have a predisposition to dysregulated neurotransmitter systems, sleep loss can exacerbate this imbalance, pushing them towards a manic state. Increased dopamine activity, for example, is associated with heightened reward sensitivity, impulsivity, and grandiosity, all hallmark symptoms of mania.
Circadian Rhythm Disruption: Our bodies operate on a 24-hour internal clock, known as the circadian rhythm, which regulates sleep-wake cycles and various physiological processes. Sleep deprivation throws this rhythm off balance, leading to desynchronization between internal and external cues. This disruption can directly impact the hypothalamic-pituitary-adrenal (HPA) axis, a key regulator of stress response. In BD-I, the HPA axis is often hypersensitive, and sleep deprivation can further activate it, leading to increased cortisol levels and a state of heightened arousal, potentially triggering mania.
Kindling Hypothesis: The kindling hypothesis proposes that repeated episodes of mood disturbance, even subthreshold ones, can lower the threshold for future episodes. Sleep deprivation, by inducing a state of heightened emotional and physiological arousal, can act as a kindling agent, making the brain more susceptible to manic switches. This means that even a single night of missed sleep might not directly cause mania in someone with BD-I, but it could increase the likelihood of an episode occurring in response to other stressors or triggers.
Glutamate Excitotoxicity: Glutamate is an excitatory neurotransmitter crucial for learning and memory. However, excessive glutamate activity can be neurotoxic. Sleep deprivation has been shown to increase glutamate levels in the brain. In BD-I, there may already be a predisposition to glutamate dysregulation. Sleep loss can exacerbate this, leading to excitotoxicity and potentially contributing to the neurobiological changes associated with mania.
Understanding these mechanisms highlights the importance of prioritizing healthy sleep hygiene in individuals with BD-I. Consistent sleep schedules, a relaxing bedtime routine, and addressing any underlying sleep disorders are crucial for preventing sleep deprivation and reducing the risk of mania onset. Additionally, recognizing the early warning signs of sleep disruption and seeking prompt intervention can help individuals with BD-I manage their condition more effectively.
Understanding Sleep Jerks: How Common Are These Sudden Movements?
You may want to see also
Explore related products






![]()
Circadian Rhythm Disruption
One of the primary mechanisms linking circadian rhythm disruption to mania in BD-I involves the dysregulation of neurotransmitter systems, particularly dopamine and norepinephrine. Sleep deprivation increases dopamine activity in the brain, which can induce euphoria, heightened energy, and reduced need for sleep—hallmark symptoms of mania. Additionally, the stress response system, regulated by the hypothalamic-pituitary-adrenal (HPA) axis, becomes hyperactive during sleep loss, leading to elevated cortisol levels. This hyperactivity further disrupts the circadian rhythm and can precipitate manic symptoms in susceptible individuals. Studies have consistently shown that even a single night of sleep deprivation can trigger manic episodes in those with BD-I, underscoring the critical role of circadian stability in mood regulation.
Behavioral and environmental factors also contribute to circadian rhythm disruption in BD-I. Irregular sleep patterns, such as staying up late or maintaining an erratic sleep schedule, can desynchronize the internal clock from external cues like light and darkness. This misalignment is particularly problematic for individuals with BD-I, as their circadian systems may already be more sensitive to perturbations. Social jet lag, a phenomenon where sleep schedules differ significantly between workdays and free days, is another common disruptor. For those with BD-I, such inconsistencies can act as a chronic stressor, increasing the likelihood of manic episodes by continually challenging the stability of their circadian rhythm.
Therapeutically, addressing circadian rhythm disruption is essential in managing BD-I. Interventions such as maintaining a consistent sleep schedule, exposure to natural light during the day, and minimizing artificial light exposure at night can help realign the circadian rhythm. Bright light therapy, particularly in the morning, has shown promise in stabilizing mood by reinforcing the natural circadian cycle. Pharmacological approaches, including melatonin supplements or mood stabilizers, may also be used to support circadian regulation. Cognitive-behavioral therapy for insomnia (CBT-I) is another effective strategy, as it targets maladaptive sleep behaviors and thought patterns that contribute to circadian disruption.
In conclusion, circadian rhythm disruption plays a pivotal role in the relationship between sleep deprivation and mania in Bipolar I Disorder. The delicate balance of the circadian system, when disturbed, can trigger neurobiological and behavioral cascades that precipitate manic episodes. Understanding this dynamic highlights the importance of sleep hygiene and circadian stability in BD-I management. By prioritizing interventions that protect and realign the circadian rhythm, individuals with BD-I can reduce their vulnerability to mania and improve overall mood stability.
Understanding REM Sleep: How Long Does It Take to Reach This Stage?
You may want to see also
Explore related products






![]()
Preventive Sleep Strategies
Sleep is a critical factor in managing bipolar disorder, particularly for individuals with Bipolar 1 Disorder, as sleep deprivation can trigger manic episodes. Implementing preventive sleep strategies is essential to stabilize mood and prevent episodes of mania. These strategies focus on creating a consistent sleep routine, optimizing the sleep environment, and addressing behaviors that interfere with rest.
One of the most effective preventive sleep strategies is establishing a strict sleep schedule. Go to bed and wake up at the same time every day, even on weekends. This helps regulate your body’s internal clock and reduces the risk of sleep disruption. Consistency reinforces your circadian rhythm, making it easier to fall asleep and stay asleep. Avoid napping during the day, especially if you struggle with insomnia, as napping can interfere with nighttime sleep and increase the likelihood of sleep deprivation, a known trigger for mania.
Creating a sleep-conducive environment is another crucial preventive sleep strategy. Ensure your bedroom is cool, dark, and quiet. Use blackout curtains, earplugs, or white noise machines to minimize disturbances. Invest in a comfortable mattress and pillows that support restful sleep. Limit exposure to screens (phones, tablets, computers) at least one hour before bed, as the blue light emitted by these devices can disrupt your circadian rhythm and delay sleep onset. Instead, engage in relaxing activities such as reading, meditation, or gentle stretching to signal to your body that it’s time to wind down.
Managing daily habits is also vital in preventive sleep strategies. Avoid stimulants like caffeine and nicotine, especially in the afternoon and evening, as they can interfere with your ability to fall asleep. Limit alcohol consumption, as it may help you fall asleep initially but disrupts sleep quality later in the night. Incorporate regular physical activity into your routine, but avoid vigorous exercise close to bedtime, as it can be stimulating. Instead, opt for calming activities like yoga or light walking in the evening to promote relaxation.
Finally, stress management plays a significant role in preventive sleep strategies. Bipolar disorder often coexists with anxiety, which can exacerbate sleep problems. Practice relaxation techniques such as deep breathing, progressive muscle relaxation, or mindfulness meditation to reduce stress and improve sleep quality. Keep a journal to track your sleep patterns and identify any triggers that disrupt your rest. If you notice persistent sleep difficulties, consult a healthcare provider or sleep specialist for personalized guidance and potential interventions, such as cognitive-behavioral therapy for insomnia (CBT-I).
By prioritizing these preventive sleep strategies, individuals with Bipolar 1 Disorder can reduce the risk of sleep deprivation and, consequently, the likelihood of mania. Consistent sleep habits, a supportive environment, healthy daily routines, and stress management are key components of a holistic approach to maintaining stability and overall well-being.
Surviving Exams: The Minimal Sleep You Need to Perform Well
You may want to see also
Explore related products





![Insomnia [Blu-ray]](https://m.media-amazon.com/images/I/91yjuJkz+ZL._AC_UY218_.jpg)
![]()
Medication & Sleep Interaction
Individuals with Bipolar 1 Disorder often rely on medications to stabilize mood and prevent manic or depressive episodes. However, the interaction between these medications and sleep patterns can significantly impact their effectiveness and side effects. Many mood stabilizers, antipsychotics, and antidepressants prescribed for Bipolar 1 Disorder can disrupt sleep architecture, either by causing insomnia or excessive sedation. For example, stimulatory effects of certain medications, such as some antidepressants or second-generation antipsychotics like aripiprazole, may interfere with the ability to fall or stay asleep. Conversely, medications like quetiapine or mirtazapine are often sedating and can lead to oversleeping or non-restorative sleep. Understanding these interactions is crucial, as sleep disturbances can exacerbate mood instability and potentially trigger manic episodes in vulnerable individuals.
Sleep deprivation is a well-documented trigger for mania in Bipolar 1 Disorder, and medication-induced sleep disturbances can inadvertently contribute to this risk. For instance, if a medication causes insomnia, the resulting sleep deprivation may lower the threshold for mania onset. This is particularly concerning because mania often begins with subtle changes in sleep patterns, such as decreased sleep need or difficulty staying asleep. Patients and clinicians must monitor sleep changes when initiating or adjusting medications to mitigate this risk. In some cases, modifying the dosage or timing of medication (e.g., taking sedating medications at night) can help minimize sleep disruption while maintaining therapeutic benefits.
On the other hand, medications that promote sleep, such as certain mood stabilizers or antipsychotics, may inadvertently mask emerging manic symptoms by normalizing sleep patterns temporarily. This can delay recognition of an impending manic episode, as sleep disturbances are often early warning signs. Patients should be educated to track not only their mood but also their sleep quality and duration, especially when starting new medications. Regular communication with healthcare providers about sleep patterns can help adjust treatment plans proactively to prevent manic episodes.
The interplay between medication side effects and sleep hygiene practices cannot be overlooked. Patients with Bipolar 1 Disorder should adopt sleep-promoting behaviors, such as maintaining a consistent sleep schedule, limiting caffeine and screen time before bed, and creating a restful sleep environment. Combining these practices with medication management can enhance sleep quality and reduce the risk of medication-induced sleep disturbances. Additionally, clinicians may consider adjunctive treatments, such as melatonin or low-dose benzodiazepines, to address sleep issues without compromising mood stability.
Finally, individualized treatment is key when managing Bipolar 1 Disorder and its interaction with sleep and medication. What works for one person may not work for another, and ongoing assessment of both mood and sleep is essential. Patients should be encouraged to keep a sleep and mood diary to identify patterns and triggers. By addressing sleep disturbances proactively and tailoring medication regimens to minimize adverse effects, the risk of mania triggered by sleep deprivation can be significantly reduced, leading to better long-term outcomes for individuals with Bipolar 1 Disorder.
Shockwave Surgery: Understanding Anesthesia and Sedation Options for Patients
You may want to see also
Frequently asked questions
Yes, sleep deprivation is a well-known trigger for manic episodes in individuals with Bipolar 1 Disorder. Even a single night of insufficient sleep can disrupt mood stability and potentially induce mania.
Sleep deprivation disrupts the brain’s regulation of mood and energy levels, which can lead to manic symptoms such as elevated mood, increased energy, irritability, and racing thoughts in people with Bipolar 1 Disorder.
Yes, maintaining a consistent sleep schedule is a crucial part of managing Bipolar 1 Disorder. Regular sleep helps stabilize mood and reduces the risk of manic episodes triggered by sleep disturbances.
If sleep deprivation occurs, it’s important to prioritize rest and seek help from a healthcare provider. They may recommend strategies like relaxation techniques, medication adjustments, or temporary sleep aids to prevent a manic episode.