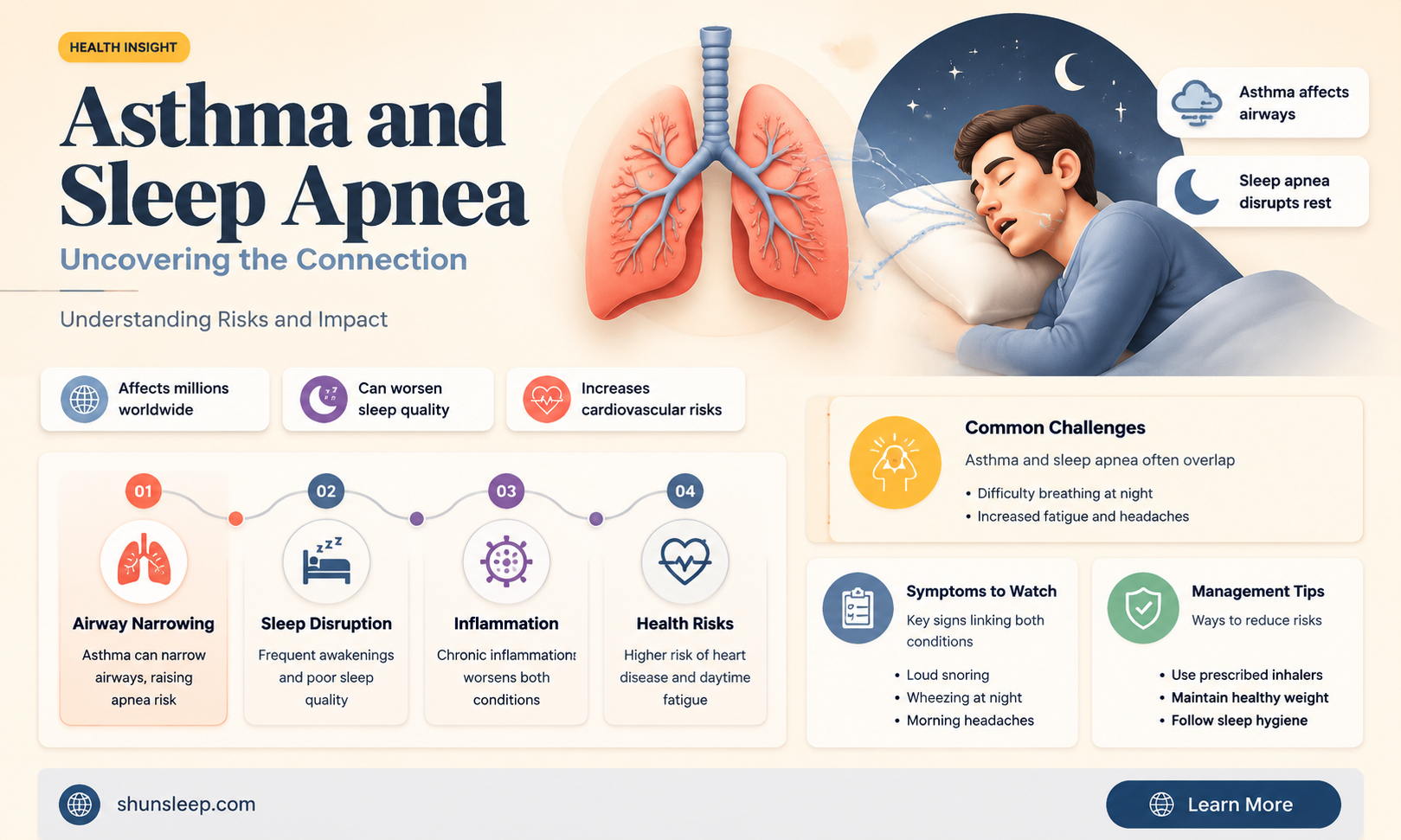
Asthma and sleep apnea are both respiratory conditions, but their relationship is often overlooked. While asthma is characterized by inflammation and narrowing of the airways, sleep apnea involves repeated interruptions in breathing during sleep, often due to airway obstruction. Recent studies suggest that individuals with asthma may be at a higher risk of developing sleep apnea, possibly due to shared underlying mechanisms such as airway inflammation and hyperresponsiveness. Understanding this connection is crucial, as untreated sleep apnea can exacerbate asthma symptoms, reduce treatment effectiveness, and negatively impact overall quality of life. This raises important questions about screening, diagnosis, and management strategies for patients with both conditions.
| Characteristics | Values |
|---|---|
| Prevalence | Asthmatics are at a higher risk of developing sleep apnea compared to the general population. Studies suggest a bidirectional relationship between asthma and sleep apnea. |
| Risk Factors | Obesity, nocturnal asthma, severe or uncontrolled asthma, and allergic rhinitis are common risk factors for sleep apnea in asthmatics. |
| Symptoms | Snoring, daytime sleepiness, morning headaches, and difficulty concentrating, along with asthma symptoms like wheezing and shortness of breath. |
| Mechanisms | Upper airway inflammation, bronchial hyperresponsiveness, and increased airway resistance contribute to the overlap between asthma and sleep apnea. |
| Diagnosis | Polysomnography (sleep study) is the gold standard for diagnosing sleep apnea in asthmatics. Asthma control should be assessed simultaneously. |
| Treatment | Continuous Positive Airway Pressure (CPAP) therapy, weight management, asthma control medications, and positional therapy are effective treatments. |
| Complications | Untreated sleep apnea in asthmatics can lead to worsened asthma control, increased hospitalizations, and cardiovascular complications. |
| Prognosis | Proper management of both conditions can improve overall quality of life and reduce the risk of complications. |
| Research | Recent studies highlight the importance of screening asthmatics for sleep apnea, especially those with severe or nocturnal symptoms. |
Explore related products






What You'll Learn
- Asthma and Sleep Apnea Link: Exploring the connection between asthma and sleep apnea prevalence
- Symptoms Overlap: Identifying shared symptoms like nighttime coughing and breathing difficulties
- Risk Factors: Common factors like obesity, allergies, and inflammation increasing dual risk
- Treatment Challenges: Managing both conditions simultaneously with medications and lifestyle adjustments
- Diagnostic Approaches: Sleep studies and lung function tests for accurate dual diagnosis
![]()
Asthma and Sleep Apnea Link: Exploring the connection between asthma and sleep apnea prevalence
The relationship between asthma and sleep apnea is a topic of growing interest in the medical community, as both conditions significantly impact respiratory health and quality of life. Research indicates that individuals with asthma may be at an increased risk of developing sleep apnea, a sleep disorder characterized by repeated interruptions in breathing during sleep. This connection is not merely coincidental but rooted in shared physiological mechanisms and risk factors. For instance, both conditions involve inflammation and narrowing of the airways, which can exacerbate symptoms and create a cycle of respiratory distress. Understanding this link is crucial for healthcare providers to offer comprehensive care and improve patient outcomes.
One of the primary factors connecting asthma and sleep apnea is the underlying airway inflammation present in both conditions. Asthma causes chronic inflammation of the airways, leading to symptoms like wheezing, shortness of breath, and coughing. Similarly, sleep apnea, particularly obstructive sleep apnea (OSA), involves inflammation and swelling of the upper airway tissues, which can collapse and block airflow during sleep. Studies suggest that the systemic inflammation in asthma may contribute to the development of OSA by increasing the susceptibility of the upper airway to collapse. Additionally, asthma-related symptoms such as coughing or bronchospasms can worsen sleep apnea episodes, creating a bidirectional relationship between the two conditions.
Another critical aspect of the asthma-sleep apnea link is the role of obesity, a common risk factor for both disorders. Obesity can exacerbate asthma symptoms by increasing airway inflammation and reducing lung function. It is also a leading risk factor for OSA, as excess fat deposits around the upper airway can narrow the passage and increase the likelihood of obstruction. Asthmatic individuals who are overweight or obese may therefore face a compounded risk of developing sleep apnea. Addressing obesity through lifestyle modifications, such as diet and exercise, can potentially mitigate this risk and improve respiratory health in patients with asthma.
The prevalence of sleep apnea in asthmatics also highlights the importance of proper diagnosis and management. Sleep apnea often goes undiagnosed, as its symptoms, such as snoring, fatigue, and daytime sleepiness, can be attributed to other conditions, including asthma itself. However, untreated sleep apnea can worsen asthma control, leading to more frequent exacerbations and reduced response to asthma medications. Healthcare providers should be vigilant in screening asthmatic patients for sleep apnea, particularly those with poorly controlled symptoms or comorbidities like obesity. Diagnostic tools such as polysomnography (sleep studies) can help confirm the presence of sleep apnea and guide appropriate treatment strategies.
Managing the coexistence of asthma and sleep apnea requires a multifaceted approach. Continuous positive airway pressure (CPAP) therapy, the gold standard treatment for OSA, can improve breathing during sleep and reduce asthma symptoms in some patients. Additionally, optimizing asthma control through the use of inhaled corticosteroids and bronchodilators is essential to minimize airway inflammation and hyperresponsiveness. Patient education plays a vital role as well, as individuals need to understand the interplay between these conditions and the importance of adhering to treatment regimens. Collaborative care involving pulmonologists, sleep specialists, and primary care physicians can ensure a holistic approach to managing both asthma and sleep apnea.
In conclusion, the link between asthma and sleep apnea is multifaceted, involving shared inflammatory pathways, common risk factors like obesity, and overlapping symptoms. Recognizing this connection is essential for early detection and effective management of both conditions. By addressing the unique challenges posed by their coexistence, healthcare providers can improve respiratory health, enhance quality of life, and reduce the burden of these prevalent disorders on patients. Further research is needed to explore the underlying mechanisms and develop targeted interventions for individuals with asthma and sleep apnea.
Do Women Suffer from Sleep Apnea? Uncovering the Hidden Truth
You may want to see also
Explore related products






![]()
Symptoms Overlap: Identifying shared symptoms like nighttime coughing and breathing difficulties
Asthma and sleep apnea are two distinct respiratory conditions, but they often share symptoms that can complicate diagnosis and treatment. One of the most notable overlaps is nighttime coughing, which is common in both conditions. In asthma, coughing at night may be triggered by airway inflammation, allergens, or cold air. In sleep apnea, coughing can occur as a reflex when the airway is partially or fully obstructed during sleep. This symptom can be particularly confusing for asthmatics, as they may attribute it solely to their asthma without considering the possibility of sleep apnea. Recognizing this overlap is crucial, as untreated sleep apnea can exacerbate asthma symptoms and vice versa.
Another shared symptom is breathing difficulties during sleep, which can manifest as gasping, wheezing, or a feeling of suffocation. Asthmatics often experience nocturnal asthma attacks, where airway constriction leads to difficulty breathing. Similarly, individuals with sleep apnea may experience repeated episodes of breathing cessation (apneas) or shallow breathing (hypopneas) due to airway obstruction. These episodes can mimic asthma symptoms, making it challenging for patients and healthcare providers to differentiate between the two conditions. Monitoring breathing patterns during sleep and noting any irregularities can help in identifying whether the issue is asthma-related or indicative of sleep apnea.
Fatigue and daytime sleepiness are additional symptoms that overlap between asthma and sleep apnea. Asthmatics may experience fatigue due to poor sleep quality caused by nighttime symptoms like coughing or wheezing. Sleep apnea sufferers also report excessive daytime sleepiness because their sleep is frequently interrupted by apneas or hypopneas. This shared symptom can lead asthmatics to overlook the possibility of sleep apnea, assuming their tiredness is solely due to their asthma. Keeping a sleep diary to track sleep quality and daytime energy levels can be a useful tool in distinguishing between the two conditions.
Snoring is another symptom that can occur in both asthmatics and individuals with sleep apnea. While snoring is more commonly associated with sleep apnea, asthmatics may also snore due to narrowed airways or increased mucus production. However, in sleep apnea, snoring is often louder and more persistent, sometimes accompanied by choking or gasping sounds. Asthmatics who snore regularly should consider the possibility of sleep apnea, especially if they experience other overlapping symptoms. Consulting a healthcare provider for a sleep study can help clarify the underlying cause of snoring.
Finally, morning headaches are a symptom that can appear in both conditions. In sleep apnea, headaches are often caused by reduced oxygen levels and increased carbon dioxide levels during apneic episodes. Asthmatics may also experience morning headaches due to poor sleep quality or nighttime asthma symptoms. This overlap further highlights the importance of a comprehensive evaluation when asthmatics present with symptoms that could be attributed to either condition. Addressing both asthma and sleep apnea is essential for improving overall respiratory health and quality of life.
Memory Foam and Health: Can It Make You Sick?
You may want to see also
Explore related products






![]()
Risk Factors: Common factors like obesity, allergies, and inflammation increasing dual risk
The relationship between asthma and sleep apnea is complex, and several common risk factors can increase the likelihood of developing both conditions. One significant factor is obesity, which plays a dual role in exacerbating both asthma and sleep apnea. Excess body weight can lead to increased inflammation and airway resistance, worsening asthma symptoms. Simultaneously, obesity is a well-known risk factor for obstructive sleep apnea (OSA), as it can cause fat deposition around the upper airway, leading to repeated collapses during sleep. For asthmatics, managing weight is crucial, as it not only reduces the severity of asthma but also lowers the risk of developing sleep apnea.
Allergies are another shared risk factor that can contribute to the dual burden of asthma and sleep apnea. Allergic reactions can trigger asthma symptoms by causing airway inflammation and constriction. In the context of sleep apnea, allergies can lead to nasal congestion and upper airway inflammation, making it harder to breathe during sleep. This is particularly problematic for asthmatics, as allergic reactions can exacerbate both conditions simultaneously. Addressing allergies through medication, environmental modifications, or immunotherapy can help mitigate these risks and improve overall respiratory health.
Inflammation is a common denominator in both asthma and sleep apnea, acting as a bridge between the two conditions. Asthma is characterized by chronic airway inflammation, which can be triggered by various factors, including allergens, infections, or irritants. Sleep apnea, particularly OSA, is also associated with systemic inflammation due to repeated episodes of hypoxia (low oxygen levels) and reoxygenation during sleep. For individuals with asthma, this chronic inflammation can further compromise airway function, increasing the risk of developing sleep apnea. Anti-inflammatory treatments, such as inhaled corticosteroids for asthma, may play a role in reducing this dual risk.
The interplay of these risk factors—obesity, allergies, and inflammation—creates a vicious cycle that can worsen both asthma and sleep apnea. For instance, obesity-induced inflammation can aggravate asthma symptoms, which in turn may increase the likelihood of developing sleep apnea. Similarly, untreated sleep apnea can lead to poor sleep quality, triggering asthma exacerbations. Recognizing and addressing these common factors is essential for asthmatics to reduce their risk of sleep apnea. Lifestyle modifications, such as weight management, allergy control, and anti-inflammatory strategies, should be integrated into comprehensive care plans for individuals with asthma to prevent or manage sleep apnea effectively.
Lastly, it is important for healthcare providers to screen asthmatics for sleep apnea, especially when these common risk factors are present. Early detection and intervention can prevent the progression of both conditions and improve quality of life. Patients should be educated about the symptoms of sleep apnea, such as snoring, daytime fatigue, and morning headaches, and encouraged to report them promptly. By targeting shared risk factors like obesity, allergies, and inflammation, asthmatics can take proactive steps to minimize their dual risk and maintain better respiratory and overall health.
Do Puppies Get Cold at Night? Tips for Cozy Puppy Sleep
You may want to see also
Explore related products





![]()
Treatment Challenges: Managing both conditions simultaneously with medications and lifestyle adjustments
Managing both asthma and sleep apnea simultaneously presents unique treatment challenges that require careful coordination of medications and lifestyle adjustments. Asthma, a chronic respiratory condition characterized by airway inflammation and bronchoconstriction, often complicates the management of sleep apnea, a disorder marked by repeated interruptions in breathing during sleep. The overlap of these conditions can exacerbate symptoms, making it essential to adopt a tailored treatment approach. One of the primary challenges is ensuring that medications for one condition do not worsen the other. For instance, some asthma medications, such as beta-agonists, may increase the risk of sleep apnea symptoms by relaxing the upper airway muscles. Conversely, certain sleep apnea treatments, like continuous positive airway pressure (CPAP) therapy, may trigger asthma symptoms if not properly adjusted.
Medication management is a critical aspect of treating both conditions concurrently. Asthma controllers, such as inhaled corticosteroids, are generally safe and effective but must be used judiciously in patients with sleep apnea. Physicians may need to monitor patients closely for any adverse effects, such as throat irritation or coughing, which could interfere with sleep apnea management. Additionally, the use of leukotriene modifiers or mast cell stabilizers may be considered to address both conditions, as they can reduce airway inflammation and bronchoconstriction without exacerbating sleep apnea. However, the interplay between medications requires a personalized approach, often involving trial and error to find the optimal balance.
Lifestyle adjustments play a pivotal role in managing both asthma and sleep apnea. Weight management is particularly important, as obesity is a common risk factor for both conditions. Adopting a healthy diet and regular exercise regimen can help reduce inflammation, improve lung function, and alleviate sleep apnea symptoms. Avoiding triggers such as allergens, pollutants, and tobacco smoke is crucial for asthma control, while also benefiting sleep apnea by reducing airway irritation. Sleep hygiene practices, including maintaining a consistent sleep schedule and creating a conducive sleep environment, are essential for managing both conditions. Elevating the head of the bed or using positional therapy can also help mitigate sleep apnea symptoms without negatively impacting asthma.
Another challenge lies in the adherence to treatment regimens, particularly for CPAP therapy in patients with both asthma and sleep apnea. Some individuals may find CPAP masks uncomfortable or experience difficulty breathing through the device, especially if their asthma is not well-controlled. In such cases, alternative treatments like oral appliances or bilevel positive airway pressure (BiPAP) machines may be considered. Patient education is vital to ensure understanding of the importance of consistent use and proper maintenance of these devices. Additionally, regular follow-ups with healthcare providers are necessary to monitor progress, adjust treatments, and address any emerging issues.
Coordinating care between pulmonologists, sleep specialists, and primary care physicians is essential for effective management of both asthma and sleep apnea. A multidisciplinary approach ensures that all aspects of the patient’s health are addressed, and treatments are integrated seamlessly. For example, a pulmonologist may focus on optimizing asthma control, while a sleep specialist tailors sleep apnea therapy to minimize respiratory discomfort. Collaborative care also facilitates the identification and management of comorbidities, such as gastroesophageal reflux disease (GERD), which can exacerbate both conditions. By working together, healthcare providers can develop a comprehensive treatment plan that improves overall quality of life for patients with asthma and sleep apnea.
In conclusion, managing both asthma and sleep apnea simultaneously requires a meticulous approach to medication management and lifestyle adjustments. The interplay between these conditions demands personalized treatment strategies that consider the unique needs of each patient. Through careful coordination of care, patient education, and ongoing monitoring, it is possible to effectively address the challenges posed by these comorbid conditions and achieve better health outcomes.
Rise and Thrive: Sleep Secrets of Early Birds Revealed
You may want to see also
Explore related products






![]()
Diagnostic Approaches: Sleep studies and lung function tests for accurate dual diagnosis
When addressing the question of whether asthmatics can develop sleep apnea, it is crucial to employ precise diagnostic approaches to ensure accurate dual diagnosis. Sleep studies, particularly polysomnography (PSG), are the gold standard for diagnosing sleep apnea. During a PSG, multiple physiological parameters are monitored, including brain waves, oxygen levels, heart rate, and breathing patterns. For asthmatics, this test is essential because it can differentiate between respiratory disturbances caused by asthma exacerbations and those indicative of sleep apnea. Additionally, PSG can identify overlapping symptoms, such as nocturnal awakenings or hypoxia, which may be attributed to either condition. A thorough analysis of the PSG data allows clinicians to determine whether the patient has obstructive sleep apnea (OSA), central sleep apnea, or a mixed form, while also assessing the impact of asthma on sleep quality.
In conjunction with sleep studies, lung function tests play a pivotal role in diagnosing asthma and evaluating its severity. Spirometry, for instance, measures airflow obstruction and bronchodilator responsiveness, which are hallmark features of asthma. For patients suspected of having both asthma and sleep apnea, spirometry helps in quantifying asthma control and ruling out other respiratory conditions that might mimic asthma symptoms. Another valuable test is the measurement of fractional exhaled nitric oxide (FeNO), which assesses airway inflammation, a key component of asthma. By integrating lung function test results with sleep study findings, clinicians can better understand the interplay between asthma and sleep apnea, ensuring a comprehensive diagnostic approach.
One challenge in diagnosing sleep apnea in asthmatics is the overlap of symptoms, such as snoring, daytime fatigue, and shortness of breath. To address this, clinicians often use portable sleep monitoring devices, such as home sleep apnea tests (HSATs), which are less comprehensive than PSG but more accessible. HSATs focus primarily on breathing patterns and oxygen saturation, providing sufficient data to diagnose OSA in many cases. However, for asthmatics, HSATs may need to be supplemented with additional information from lung function tests to avoid misdiagnosis. For example, nocturnal symptoms like coughing or wheezing, which are common in asthma, could be misinterpreted as OSA-related events without proper context from lung function assessments.
A multidisciplinary approach is often necessary for accurate dual diagnosis. Pulmonologists and sleep specialists may collaborate to interpret test results and develop a tailored treatment plan. In some cases, a therapeutic trial of continuous positive airway pressure (CPAP) or bilevel positive airway pressure (BiPAP) may be initiated based on sleep study findings, while asthma management is optimized through inhaled corticosteroids or bronchodilators. Follow-up assessments, including repeat lung function tests and sleep studies, are critical to monitor treatment efficacy and adjust interventions as needed. This iterative process ensures that both conditions are effectively managed, improving overall patient outcomes.
In conclusion, diagnosing sleep apnea in asthmatics requires a meticulous combination of sleep studies and lung function tests. Polysomnography and portable sleep monitoring devices provide essential insights into sleep-related breathing disorders, while spirometry, FeNO measurements, and other lung function assessments clarify asthma’s role in the patient’s symptoms. By integrating these diagnostic tools and adopting a multidisciplinary approach, clinicians can achieve an accurate dual diagnosis, paving the way for targeted and effective treatment strategies. This comprehensive methodology is vital for addressing the complex interplay between asthma and sleep apnea, ultimately enhancing patients’ quality of life.
Fixing Windows 10 Home WiFi Issues After Sleep Mode: A Guide
You may want to see also
Frequently asked questions
Yes, asthmatics can develop sleep apnea. The two conditions often coexist due to shared risk factors like obesity, inflammation, and airway hyperresponsiveness.
Asthma can worsen sleep apnea symptoms because airway inflammation and bronchoconstriction in asthma may exacerbate upper airway obstruction during sleep.
Proper asthma management, such as using inhaled corticosteroids to reduce airway inflammation, may help alleviate some sleep apnea symptoms, but sleep apnea often requires separate treatment like CPAP therapy.