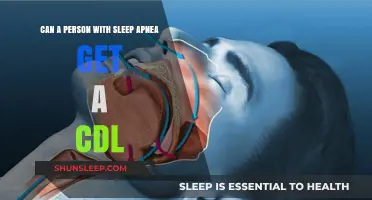
Sleep apnea, a condition characterized by pauses in breathing during sleep, is often associated with adults, but it can also affect young children, including 2-year-olds. While less common in this age group, sleep apnea in toddlers can arise from various factors such as enlarged tonsils or adenoids, obesity, or underlying medical conditions. Symptoms may include loud snoring, restless sleep, mouth breathing, and daytime fatigue, which can impact a child’s growth, behavior, and cognitive development. Early recognition and consultation with a pediatrician are crucial to diagnose and address the condition, ensuring the child receives appropriate treatment to improve their sleep quality and overall health.
| Characteristics | Values |
|---|---|
| Prevalence | Sleep apnea is relatively rare in 2-year-olds but can occur. Estimates suggest 1-4% of toddlers may experience sleep-disordered breathing. |
| Types | - Obstructive Sleep Apnea (OSA): Most common in this age group, caused by enlarged tonsils/adenoids or anatomical abnormalities. - Central Sleep Apnea: Less common, involves the brain failing to signal muscles to breathe. |
| Risk Factors | - Enlarged tonsils/adenoids - Obesity - Family history of sleep apnea - Premature birth - Down syndrome or other genetic conditions - Allergies or chronic nasal congestion |
| Symptoms | - Loud snoring - Pauses in breathing during sleep - Restless sleep, frequent awakenings - Mouth breathing - Daytime sleepiness or irritability - Bedwetting - Failure to thrive (poor weight gain) |
| Diagnosis | - Sleep study (polysomnography) - Physical examination by a pediatrician or ENT specialist |
| Treatment | - Adenotonsillectomy: Surgical removal of tonsils/adenoids (most common treatment) - CPAP/BiPAP therapy (in severe cases) - Allergy management - Weight management (if applicable) |
| Complications (if untreated) | - Cognitive and behavioral issues - Growth and developmental delays - Cardiovascular problems - Increased risk of accidents due to daytime sleepiness |
| Prognosis | Generally good with appropriate treatment. Most children outgrow OSA after adenotonsillectomy. |
Explore related products






What You'll Learn
- Symptoms in Toddlers: Snoring, restless sleep, pauses in breathing, mouth breathing, and daytime fatigue
- Common Causes: Enlarged tonsils, adenoids, allergies, obesity, or genetic conditions
- Diagnosis Methods: Sleep studies, physical exams, and medical history evaluation
- Treatment Options: Surgery, allergy management, weight control, or CPAP therapy
- Long-Term Effects: Behavioral issues, growth delays, cognitive problems, and cardiovascular risks
![]()
Symptoms in Toddlers: Snoring, restless sleep, pauses in breathing, mouth breathing, and daytime fatigue
Sleep apnea, though more commonly associated with adults, can indeed affect toddlers, including 2-year-olds. Recognizing the symptoms early is crucial for timely intervention. One of the most noticeable signs is snoring, which is often dismissed as harmless in children. However, loud, frequent, or habitual snoring in a toddler could indicate obstructed airflow, a hallmark of sleep apnea. Unlike occasional snoring due to a cold or allergies, sleep apnea-related snoring persists and may be accompanied by gasping or choking sounds during sleep.
Another key symptom is restless sleep. Toddlers with sleep apnea often exhibit frequent tossing and turning, difficulty staying in one position, or even sitting up during sleep to breathe more easily. This restlessness occurs because their bodies are constantly trying to overcome the airway obstruction, preventing them from achieving deep, restorative sleep. Parents may notice their child appears uncomfortable or unsettled throughout the night, even if they don’t fully wake up.
Pauses in breathing are a particularly alarming symptom of sleep apnea in toddlers. These pauses, known as apneas, can last for several seconds and may be followed by sudden gasping or snorting as the child resumes breathing. Observing these episodes can be distressing for parents, but they are a clear indicator that the child’s airway is being compromised. If such pauses occur regularly, it’s essential to consult a pediatrician promptly.
Mouth breathing is another common symptom in toddlers with sleep apnea. Since their nasal passages may be obstructed due to enlarged tonsils, adenoids, or other factors, they rely on mouth breathing to get enough air. Chronic mouth breathing can lead to dry lips, drooling, or even changes in facial development over time. Parents may also notice their child’s mouth hanging open during sleep or even while awake.
Lastly, daytime fatigue is a significant red flag in toddlers with sleep apnea. Despite seemingly sleeping through the night, these children often appear excessively tired, irritable, or hyperactive during the day. This is because their sleep is fragmented and of poor quality, leaving them unable to recharge properly. Daytime fatigue may also manifest as difficulty concentrating, poor appetite, or behavioral issues, which can sometimes be mistaken for developmental or disciplinary problems. If a 2-year-old consistently shows signs of exhaustion despite adequate sleep hours, sleep apnea should be considered as a potential cause.
In summary, while sleep apnea in toddlers can be concerning, early recognition of symptoms like snoring, restless sleep, pauses in breathing, mouth breathing, and daytime fatigue can lead to effective management. Parents who observe these signs in their 2-year-old should seek medical advice to ensure their child receives the necessary care and treatment.
Do Guys Form Emotional Attachments After Intimacy? Exploring the Truth
You may want to see also
Explore related products






![]()
Common Causes: Enlarged tonsils, adenoids, allergies, obesity, or genetic conditions
Sleep apnea in 2-year-olds, though less common than in adults, can occur and is often linked to specific underlying causes. One of the most frequent contributors is enlarged tonsils and adenoids. At this age, these lymphatic tissues are still developing and can become disproportionately large relative to the child’s airway. When tonsils and adenoids swell—often due to recurrent infections or inflammation—they can obstruct the upper airway, leading to disrupted breathing during sleep. This condition, known as obstructive sleep apnea (OSA), is characterized by snoring, pauses in breathing, and restless sleep. Parents may notice their child sleeping in unusual positions, such as with their neck hyperextended, as they unconsciously try to open their airway.
Allergies are another common cause of sleep apnea in 2-year-olds. Allergic reactions can lead to nasal congestion, inflammation, and swelling of the airway tissues, making it harder for a child to breathe freely during sleep. Seasonal allergies, dust mites, pet dander, or food allergies can all contribute to this issue. Chronic nasal congestion forces children to breathe through their mouths, which can exacerbate airway obstruction and increase the likelihood of apnea episodes. Parents may observe symptoms like persistent sniffling, rubbing of the nose, or mouth breathing during the day, which often worsen at night.
Obesity is a growing concern in pediatric sleep apnea, even in toddlers. Excess weight can lead to the accumulation of fatty tissue around the neck and throat, narrowing the airway and increasing the risk of obstruction. While obesity is less common in 2-year-olds compared to older children, early childhood weight issues—often influenced by diet and lifestyle—can still play a role. Parents should monitor their child’s growth patterns and consult a pediatrician if they suspect weight-related health concerns. Addressing obesity through dietary changes and increased physical activity can help alleviate sleep apnea symptoms.
Genetic conditions can also predispose 2-year-olds to sleep apnea. Disorders such as Down syndrome, Pierre Robin sequence, or other craniofacial abnormalities often result in structural abnormalities of the airway, making it more susceptible to collapse during sleep. These conditions may cause a smaller jaw, recessed chin, or a tongue that sits farther back in the mouth, all of which can contribute to airway obstruction. Children with genetic syndromes often require specialized care, including evaluations by ENT specialists, pulmonologists, or geneticists, to manage sleep apnea effectively.
In summary, sleep apnea in 2-year-olds is often rooted in enlarged tonsils and adenoids, allergies, obesity, or genetic conditions. Recognizing the signs—such as snoring, labored breathing, or daytime sleepiness—is crucial for early intervention. Parents should consult a healthcare provider if they suspect their child is experiencing sleep-disordered breathing. Treatment may involve allergy management, surgical removal of tonsils and adenoids (adenotonsillectomy), weight management, or addressing underlying genetic factors. Timely diagnosis and treatment can prevent long-term complications, such as developmental delays or cardiovascular issues, and ensure healthy sleep patterns for the child.
Sleepless Nights, Agitated Days: The Impact of Sleep Deprivation on Mood
You may want to see also
Explore related products






![]()
Diagnosis Methods: Sleep studies, physical exams, and medical history evaluation
Diagnosing sleep apnea in 2-year-olds requires a careful and multifaceted approach, as young children may not exhibit symptoms as clearly as adults. Sleep studies, particularly polysomnography (PSG), are considered the gold standard for diagnosis. During a PSG, the child’s brain waves, heart rate, oxygen levels, breathing patterns, and body movements are monitored overnight in a sleep lab or at home with portable equipment. For toddlers, this process is adapted to be as non-invasive and child-friendly as possible, often involving stickers or small sensors placed on the skin. The study helps identify pauses in breathing, oxygen desaturation, and other abnormalities characteristic of sleep apnea. However, conducting a PSG in young children can be challenging due to their restlessness and shorter sleep cycles, so specialized pediatric sleep centers are often recommended.
Physical exams play a crucial role in identifying potential causes of sleep apnea in 2-year-olds. Pediatricians will examine the child’s airway for structural abnormalities, such as enlarged tonsils or adenoids, which are common culprits in pediatric sleep apnea. Other physical signs, like a recessed chin, narrow jaw, or obesity, may also be assessed. In some cases, a referral to an ear, nose, and throat (ENT) specialist may be necessary for a more detailed evaluation of the upper airway. It’s important for parents to note any visible symptoms during sleep, such as snoring, gasping, or choking, as these observations can guide the physical examination.
Medical history evaluation is another critical component of diagnosing sleep apnea in toddlers. Parents or caregivers will be asked to provide detailed information about the child’s sleep patterns, including snoring frequency, restlessness, and daytime behaviors like irritability, hyperactivity, or difficulty concentrating. A history of respiratory infections, allergies, or premature birth may also be relevant, as these factors can contribute to airway issues. Additionally, family history of sleep disorders or obesity can provide valuable insights. This comprehensive evaluation helps clinicians determine whether further testing is needed and tailor the diagnostic approach to the child’s specific needs.
In some cases, additional diagnostic tools may be employed to complement sleep studies, physical exams, and medical history evaluations. For instance, a nasal endoscopy or imaging studies like X-rays or MRIs may be used to visualize the airway and identify structural issues. However, these methods are typically reserved for complex cases or when initial evaluations are inconclusive. The primary focus remains on non-invasive, child-friendly techniques that minimize stress for both the toddler and their caregivers.
Early and accurate diagnosis of sleep apnea in 2-year-olds is essential, as untreated sleep disorders can lead to developmental delays, behavioral issues, and long-term health problems. By combining sleep studies, thorough physical exams, and detailed medical history evaluations, healthcare providers can effectively identify and address sleep apnea in young children, ensuring they receive the appropriate treatment and support for healthy sleep and overall well-being.
Accessing Your Sleep Report from System One: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Treatment Options: Surgery, allergy management, weight control, or CPAP therapy
While sleep apnea is more commonly associated with adults, it can indeed affect young children, including 2-year-olds. The treatment approach for pediatric sleep apnea often involves addressing the underlying cause, which may include enlarged tonsils or adenoids, allergies, obesity, or other anatomical abnormalities. Here are the primary treatment options tailored for toddlers:
Surgery is often the first-line treatment for 2-year-olds with sleep apnea, particularly when enlarged tonsils or adenoids are the primary cause. Adenotonsillectomy, the surgical removal of both the adenoids and tonsils, is a common and effective procedure. It can significantly improve breathing during sleep and resolve symptoms like snoring, pauses in breathing, and restless sleep. Pediatric ENT specialists typically perform this procedure, and while it involves a short recovery period, it is generally safe and highly successful in alleviating sleep apnea in young children.
Allergy management plays a crucial role if allergies contribute to sleep apnea in toddlers. Allergic reactions can cause nasal congestion and inflammation, narrowing the airway and exacerbating breathing difficulties during sleep. Treatment may include identifying and avoiding allergens, using antihistamines, or administering nasal corticosteroids to reduce inflammation. In some cases, allergy immunotherapy (allergy shots) may be recommended to desensitize the child to specific allergens over time. Addressing allergies can improve overall sleep quality and reduce apnea episodes.
Weight control is another important consideration, though it is less common in 2-year-olds compared to older children. If a toddler is overweight, this can contribute to sleep apnea by placing extra pressure on the airway. Pediatricians may recommend a balanced diet and age-appropriate physical activities to promote healthy weight management. Even modest weight reduction can improve symptoms and overall health in affected children.
CPAP therapy (Continuous Positive Airway Pressure) is generally reserved for cases where surgery is not an option or as a temporary measure. CPAP involves wearing a mask that delivers a steady stream of air to keep the airway open during sleep. However, CPAP can be challenging to implement in toddlers due to their age and difficulty tolerating the mask. It is typically considered only after other treatments have been explored and under close medical supervision.
In summary, the treatment of sleep apnea in 2-year-olds is multifaceted and depends on the underlying cause. Surgery is often the most effective solution for anatomical issues, while allergy management and weight control address contributing factors. CPAP therapy remains a last resort due to its practical challenges in young children. Early diagnosis and intervention are key to ensuring healthy sleep and overall development in toddlers with sleep apnea.
Can You Catch STIs from Sleeping with One Partner?
You may want to see also
Explore related products






![]()
Long-Term Effects: Behavioral issues, growth delays, cognitive problems, and cardiovascular risks
Sleep apnea in 2-year-olds, though less common than in adults, can have significant long-term effects if left untreated. One of the most concerning areas is behavioral issues. Chronic sleep disruption caused by apnea can lead to irritability, hyperactivity, and difficulty regulating emotions. Toddlers with untreated sleep apnea may exhibit aggressive behavior, temper tantrums, or difficulty focusing, which can mimic symptoms of attention-deficit/hyperactivity disorder (ADHD). These behavioral challenges can strain family dynamics and hinder social development, as the child may struggle to interact with peers or follow routines in daycare or preschool settings.
Growth delays are another critical long-term consequence of sleep apnea in young children. During deep sleep, the body releases growth hormone, which is essential for physical development. Sleep apnea disrupts this process, leading to poor weight gain, stunted height, and delayed milestones. For a 2-year-old, this could mean falling behind in motor skills, such as walking or running, or failing to meet expected growth charts. Addressing sleep apnea early is crucial to ensure proper physical development and prevent long-term growth impairments.
Cognitive problems are also a significant risk for toddlers with untreated sleep apnea. Quality sleep is vital for brain development, particularly in areas like memory, problem-solving, and language acquisition. Chronic sleep deprivation can impair these functions, leading to learning difficulties, delayed speech, and poor academic performance later in life. Studies suggest that children with sleep apnea may struggle with concentration, have lower IQ scores, and face challenges in school compared to their peers. Early intervention is key to mitigating these cognitive risks and supporting healthy brain development.
Lastly, cardiovascular risks should not be overlooked, even in very young children. Sleep apnea can strain the cardiovascular system by causing intermittent hypoxia (low oxygen levels) and increased blood pressure. Over time, this can lead to hypertension, abnormal heart rhythms, or even structural heart problems. While these risks are more commonly associated with adults, research indicates that untreated sleep apnea in childhood can lay the groundwork for cardiovascular issues later in life. Parents and caregivers must recognize the importance of addressing sleep apnea to protect their child’s long-term heart health.
In summary, sleep apnea in 2-year-olds is not just a minor sleep disturbance—it can have profound and lasting effects on a child’s behavioral, physical, cognitive, and cardiovascular health. Early diagnosis and treatment, such as addressing enlarged tonsils or adenoids, using continuous positive airway pressure (CPAP) therapy, or making lifestyle changes, are essential to prevent these long-term complications. Parents and healthcare providers must remain vigilant and proactive in ensuring that young children receive the quality sleep they need for healthy development.
Does IBS Worsen at Night? Understanding Sleep and Symptoms
You may want to see also
Frequently asked questions
Yes, 2-year-olds can develop sleep apnea, though it is less common than in adults. Pediatric sleep apnea often results from enlarged tonsils or adenoids, allergies, or structural abnormalities in the airway.
Common signs include loud snoring, pauses in breathing during sleep, restless sleep, mouth breathing, bedwetting, and daytime symptoms like irritability, hyperactivity, or difficulty concentrating.
Treatment depends on the cause. Common approaches include removing enlarged tonsils or adenoids (adenotonsillectomy), managing allergies, or using continuous positive airway pressure (CPAP) in severe cases. Consult a pediatrician or sleep specialist for evaluation and guidance.