Hypnograms, graphical representations of sleep stages over time, play a crucial role in diagnosing sleep disorders by providing detailed insights into an individual’s sleep architecture. By tracking transitions between wakefulness, light sleep, deep sleep, and REM sleep, hypnograms help identify abnormalities such as fragmented sleep, reduced deep sleep, or excessive awakenings, which are hallmark indicators of conditions like insomnia, sleep apnea, or restless leg syndrome. Clinicians use these visual tools to assess sleep quality, detect disruptions in sleep cycles, and tailor treatment plans, making hypnograms an invaluable diagnostic aid in sleep medicine.
| Characteristics | Values |
|---|---|
| Definition | A hypnogram is a graphical representation of sleep stages over time, generated from polysomnography (PSG) data. |
| Sleep Stages Monitored | Tracks stages: Wake, N1 (light sleep), N2 (moderate sleep), N3 (deep sleep), and REM (rapid eye movement) sleep. |
| Diagnostic Utility | Helps diagnose sleep disorders by identifying abnormalities in sleep architecture, such as reduced deep sleep or excessive awakenings. |
| Disorders Identified | Insomnia, sleep apnea, narcolepsy, restless leg syndrome, circadian rhythm disorders, and parasomnias. |
| Quantitative Analysis | Provides metrics like sleep latency, total sleep time, sleep efficiency, and time spent in each stage. |
| Limitations | Requires PSG, which is costly and time-consuming; cannot diagnose disorders solely based on hypnogram without clinical context. |
| Complementary Tool | Used alongside patient history, physical exams, and other tests for comprehensive diagnosis. |
| Advancements | Modern hypnograms use automated scoring algorithms, improving accuracy and reducing reliance on manual interpretation. |
| Research Applications | Valuable in sleep research to study sleep patterns in various populations and conditions. |
| Patient Education | Helps patients visualize their sleep issues, aiding in understanding and adherence to treatment plans. |
Explore related products



$324.89 $379.99



What You'll Learn
- Hypnogram Basics: Understanding sleep stages and their representation in hypnograms
- Identifying Sleep Disorders: How hypnograms detect abnormalities like insomnia or apnea
- Hypnogram Accuracy: Reliability and limitations in diagnosing sleep disorders
- Clinical Applications: Using hypnograms in sleep disorder diagnosis and treatment planning
- Comparing Hypnograms: Differentiating normal sleep patterns from disordered sleep via hypnograms
![]()
Hypnogram Basics: Understanding sleep stages and their representation in hypnograms
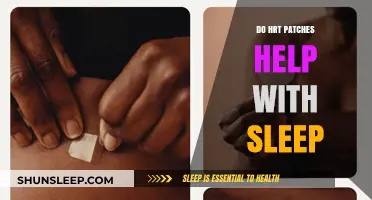
Sleep is a complex process, divided into distinct stages that cycle throughout the night. A hypnogram, a graphical representation of these stages, serves as a critical tool in sleep analysis. It plots sleep stages—Wake, N1, N2, N3 (deep sleep), and REM—over time, offering a visual snapshot of sleep architecture. Each stage is identified through electroencephalogram (EEG) readings, which measure brain wave patterns. For instance, N1 and N2 show lighter sleep with higher frequency waves, while N3 displays slow delta waves, indicating deep restorative sleep. REM sleep, marked by rapid eye movements and vivid dreams, is characterized by brain activity resembling wakefulness. Understanding these stages is foundational to interpreting hypnograms and identifying potential sleep disorders.
Consider the hypnogram as a roadmap of the night’s sleep. A healthy sleep pattern typically shows 4–5 cycles, each lasting 90–120 minutes, with REM sleep increasing in duration toward morning. However, deviations from this pattern can signal issues. For example, fragmented sleep, where multiple awakenings disrupt the cycle, or reduced deep sleep (N3) may indicate insomnia or sleep apnea. Similarly, an overabundance of light sleep (N1, N2) could suggest restless leg syndrome or periodic limb movement disorder. Hypnograms also highlight abnormalities like REM sleep behavior disorder, where REM sleep intrudes into other stages, leading to physical acting out of dreams. By analyzing these patterns, clinicians can pinpoint disruptions and tailor interventions.
Interpreting a hypnogram requires both technical knowledge and clinical insight. For instance, a patient with narcolepsy might show REM sleep occurring abnormally early in the sleep cycle, a phenomenon known as SOREMP (Sleep Onset REM Period). Conversely, someone with sleep apnea may exhibit frequent arousals, disrupting the progression into deeper sleep stages. Practical tips for patients include maintaining a consistent sleep schedule and avoiding stimulants before bed to improve sleep continuity. For clinicians, correlating hypnogram data with patient symptoms—such as daytime fatigue or snoring—enhances diagnostic accuracy. Tools like the Sleep Fragmentation Index, derived from hypnogram data, quantify disruptions and aid in treatment planning.
While hypnograms are invaluable, they are not without limitations. They rely on polysomnography, an overnight sleep study, which can be costly and inaccessible for some patients. Additionally, hypnograms provide a macro view of sleep architecture but lack the granularity to diagnose conditions like circadian rhythm disorders, which require actigraphy or melatonin assays. Despite these constraints, hypnograms remain a cornerstone in sleep medicine, bridging the gap between subjective patient reports and objective data. By mastering their interpretation, healthcare providers can better identify sleep disorders and improve patient outcomes, ensuring that each night’s rest contributes to overall health.
Shed Pounds Despite Sleep Deprivation: Strategies for Weight Loss Success
You may want to see also
Explore related products






![]()
Identifying Sleep Disorders: How hypnograms detect abnormalities like insomnia or apnea
Hypnograms, visual representations of sleep stages over time, serve as critical tools in diagnosing sleep disorders by revealing patterns that deviate from normal sleep architecture. These graphs plot sleep cycles across the night, showing transitions between wakefulness, light sleep, deep sleep, and REM sleep. In a healthy individual, a hypnogram typically displays a balanced distribution of these stages, with deep sleep dominating the early night and REM sleep increasing toward morning. However, abnormalities in this pattern often signal underlying disorders. For instance, fragmented sleep with frequent awakenings may indicate insomnia, while a near-absence of deep sleep could suggest sleep apnea. By analyzing these deviations, clinicians can pinpoint specific disruptions in sleep structure, guiding targeted interventions.
Consider the case of obstructive sleep apnea (OSA), a disorder characterized by repeated breathing interruptions during sleep. A hypnogram for someone with OSA often shows reduced or absent deep sleep stages, despite total sleep time appearing normal. This occurs because apneic events fragment sleep, preventing the individual from achieving restorative deep sleep. Additionally, the hypnogram may reveal a higher proportion of light sleep and frequent arousals, which are not consciously remembered but disrupt sleep quality. For adults aged 18–65, who typically require 13–23% of their sleep in the deep stage, a hypnogram showing less than 10% deep sleep warrants further investigation. Pairing hypnogram analysis with polysomnography data, such as oxygen desaturation levels, strengthens the diagnosis and informs treatment, like CPAP therapy or positional adjustments.
In contrast, insomnia manifests differently on a hypnogram, often showing prolonged periods of wakefulness or an overrepresentation of light sleep stages. For example, a middle-aged individual with chronic insomnia might spend 30–40% of their night in stage 1 sleep, compared to the typical 2–5%. This imbalance reflects difficulty transitioning to deeper sleep stages, a hallmark of the disorder. Cognitive behavioral therapy for insomnia (CBT-I) can then be tailored to address these specific disruptions, such as sleep restriction or stimulus control techniques. Hypnograms also help track treatment efficacy; improvements in sleep continuity and stage distribution post-therapy validate the intervention’s success.
While hypnograms are invaluable, their interpretation requires expertise and context. For instance, older adults naturally experience less deep sleep due to age-related changes, so a reduced deep sleep percentage in a 70-year-old might not indicate apnea. Similarly, medications like antidepressants can alter sleep architecture, mimicking disordered patterns. Clinicians must cross-reference hypnogram data with patient history, symptoms, and other diagnostic tools to avoid misdiagnosis. Practical tips for patients include maintaining a consistent sleep schedule and avoiding stimulants before bed, as these factors can influence hypnogram results. When used judiciously, hypnograms transform sleep disorder diagnosis from guesswork into a precise science, enabling personalized and effective treatment strategies.
Relax and Rest: Effective Ways to Release Tension for Better Sleep
You may want to see also
Explore related products




![]()
Hypnogram Accuracy: Reliability and limitations in diagnosing sleep disorders
Hypnograms, visual representations of sleep stages over time, are invaluable tools in sleep medicine, offering insights into sleep architecture. However, their accuracy in diagnosing sleep disorders hinges on several factors, including the quality of data collection and interpretation. Polysomnography (PSG), the gold standard for sleep studies, generates hypnograms by analyzing electroencephalogram (EEG), electromyogram (EMG), and electrooculogram (EOG) data. While PSG provides comprehensive information, the accuracy of the resulting hypnogram depends on the expertise of the scorer and the consistency of scoring criteria. For instance, the American Academy of Sleep Medicine (AASM) scoring manual standardizes sleep stage classification, but inter-rater variability remains a challenge, with studies showing discrepancies of up to 10% in stage identification.
Consider the case of obstructive sleep apnea (OSA), where hypnograms often reveal frequent arousals and fragmented sleep. While these patterns are indicative, they are not diagnostic on their own. A hypnogram may show reduced rapid eye movement (REM) sleep, a common finding in OSA, but this could also result from other conditions like depression or medication use. Thus, hypnograms serve as a piece of the diagnostic puzzle, requiring integration with clinical history, symptom severity, and other test results. For example, a patient with excessive daytime sleepiness and a hypnogram showing disrupted sleep might undergo additional testing, such as an apnea-hypopnea index (AHI) measurement, to confirm OSA.
Despite their utility, hypnograms have limitations. One significant issue is the reliance on visual interpretation, which can introduce subjectivity. Automated scoring algorithms, while improving, still struggle with complex sleep patterns, such as those seen in patients with narcolepsy or periodic limb movement disorder. Additionally, hypnograms provide a snapshot of a single night’s sleep, which may not capture chronic sleep disturbances. For instance, a patient with insomnia might exhibit normal sleep architecture on a hypnogram due to "first-night effect," where anxiety in a sleep lab improves sleep temporarily. To mitigate this, clinicians often recommend multiple-night studies or home sleep apnea tests (HSATs) for more accurate data.
Practical tips for enhancing hypnogram reliability include ensuring proper electrode placement during PSG to minimize artifact interference and using validated scoring software. Clinicians should also correlate hypnogram findings with patient-reported symptoms and actigraphy data, which tracks movement to assess sleep-wake patterns over days or weeks. For pediatric populations, age-specific norms are critical, as sleep architecture varies significantly between children and adults. For example, infants spend approximately 50% of their sleep in REM, compared to 20-25% in adults, making misdiagnosis more likely without age-adjusted interpretation.
In conclusion, hypnograms are powerful diagnostic tools when used judiciously. Their reliability stems from standardized scoring protocols and integration with other diagnostic modalities, but limitations like scorer variability and single-night data collection must be acknowledged. By combining hypnogram analysis with clinical context and complementary tests, healthcare providers can more accurately diagnose sleep disorders and tailor treatment plans. For instance, cognitive-behavioral therapy for insomnia (CBT-I) might be recommended for a patient with a hypnogram showing prolonged sleep onset latency, supported by a sleep diary documenting chronic insomnia symptoms. Ultimately, hypnograms are not standalone solutions but essential components of a comprehensive sleep evaluation.
Can You Permanently Get Stuck in Sleep? Unraveling the Myth
You may want to see also
Explore related products






![]()
Clinical Applications: Using hypnograms in sleep disorder diagnosis and treatment planning
Hypnograms, graphical representations of sleep stages over time, serve as indispensable tools in the clinical assessment of sleep disorders. By visually mapping transitions between wakefulness, rapid eye movement (REM), and non-REM sleep, they provide a quantitative foundation for diagnosing conditions like insomnia, sleep apnea, and narcolepsy. For instance, a fragmented hypnogram with frequent awakenings may indicate insomnia, while a collapsed REM latency could suggest narcolepsy. These patterns allow clinicians to move beyond subjective patient reports, grounding diagnoses in objective data.
In treatment planning, hypnograms offer a dynamic roadmap for tailoring interventions. For patients with obstructive sleep apnea, a hypnogram revealing prolonged REM deprivation can justify the prescription of continuous positive airway pressure (CPAP) therapy, often set at 10–12 cm H2O initially, adjusted based on follow-up hypnogram improvements. Similarly, cognitive behavioral therapy for insomnia (CBT-I) may be paired with sleep hygiene adjustments if a hypnogram shows excessive light sleep or early-morning awakenings. The ability to track pre- and post-treatment hypnograms ensures interventions are evidence-based and responsive to individual needs.
However, interpreting hypnograms requires caution. Artifacts from movement or sensor misplacement can distort data, leading to misdiagnosis. Clinicians must cross-reference hypnogram findings with polysomnography (PSG) metrics, such as apnea-hypopnea index (AHI) or REM density, to ensure accuracy. For pediatric cases, age-specific norms are critical; a 10-year-old’s hypnogram, for example, should show more deep sleep (stage N3) than an adult’s, reflecting developmental differences.
Despite limitations, hypnograms remain a cornerstone of sleep medicine, bridging diagnostic precision and personalized care. Their utility extends to monitoring treatment efficacy, such as tracking increased REM consolidation in patients on antidepressants for REM sleep behavior disorder. By integrating hypnogram analysis into clinical practice, providers can deliver targeted therapies, improve patient outcomes, and foster a deeper understanding of sleep architecture’s role in health and disease.
Wake Up Flawless: Quick Fixes for Overnight Sleep Impressions
You may want to see also
Explore related products

$24.99





![]()
Comparing Hypnograms: Differentiating normal sleep patterns from disordered sleep via hypnograms
Hypnograms, graphical representations of sleep stages over time, serve as critical tools in distinguishing between normal and disordered sleep patterns. A typical hypnogram for a healthy adult shows a cyclical progression through non-rapid eye movement (NREM) stages (N1, N2, N3) and rapid eye movement (REM) sleep, repeating approximately every 90 minutes. For instance, deep N3 sleep, essential for restorative functions, should constitute about 20–25% of total sleep in young adults, gradually decreasing with age. Deviations from this pattern, such as fragmented cycles or reduced N3 sleep, often signal underlying sleep disorders.
Analyzing hypnograms requires a keen eye for abnormalities. In insomnia, for example, the hypnogram may reveal prolonged wakefulness during the night, reduced sleep efficiency (below 85%), or an irregular sleep architecture with frequent shifts between stages. Conversely, in sleep apnea, the hypnogram often shows repeated arousals from deep sleep, leading to a higher proportion of lighter N1 and N2 stages and minimal REM sleep. These disruptions correlate with the patient’s symptoms, such as daytime fatigue or cognitive impairment, providing objective evidence for diagnosis.
To effectively compare hypnograms, clinicians must consider age-related norms. For instance, older adults naturally experience less N3 sleep and more awakenings, which should not be misinterpreted as pathological. However, when a 65-year-old’s hypnogram shows less than 10% N3 sleep alongside excessive daytime sleepiness, it may indicate a disorder like sleep apnea or periodic limb movement disorder. Practical tips for interpretation include focusing on sleep latency (ideally under 30 minutes), REM latency (typically 60–90 minutes), and the distribution of sleep stages relative to age-specific benchmarks.
Persuasively, hypnograms offer a non-invasive, data-driven approach to diagnosing sleep disorders, but their utility hinges on proper context. For example, a patient with narcolepsy may exhibit REM sleep within 15 minutes of sleep onset, a hallmark of the disorder. However, relying solely on hypnograms without correlating them with patient history or other tests, such as the Epworth Sleepiness Scale or polysomnography, can lead to misdiagnosis. Thus, while hypnograms are invaluable, they are most effective as part of a comprehensive sleep assessment.
In conclusion, comparing hypnograms to differentiate normal from disordered sleep requires a structured approach. Start by identifying key metrics like sleep stage distribution and cycle continuity. Next, cross-reference these findings with age-specific norms and patient symptoms. Finally, integrate the hypnogram data with other diagnostic tools to confirm or rule out sleep disorders. By mastering this process, clinicians can leverage hypnograms to provide tailored interventions, improving sleep health and overall quality of life.
Can You Still Score Sleep No More Tickets? A Guide
You may want to see also
Frequently asked questions
A hypnogram is a graphical representation of sleep stages over time, generated from a polysomnography (sleep study). It helps identify disruptions in sleep patterns, which can indicate disorders like insomnia, sleep apnea, or restless leg syndrome.
A hypnogram alone cannot diagnose a sleep disorder but provides valuable data for clinicians. It must be interpreted alongside other sleep study metrics and patient symptoms to determine a diagnosis.
A hypnogram tracks wakefulness, light sleep (N1, N2), deep sleep (N3), and REM sleep. Abnormalities in these stages, such as reduced deep sleep or fragmented REM, can suggest disorders like sleep apnea or narcolepsy.
Hypnograms are primarily used for disorders involving sleep architecture, such as insomnia, circadian rhythm disorders, or parasomnias. They are less relevant for conditions like sleep apnea, where other metrics (e.g., apnea-hypopnea index) are more critical.
Hypnograms are highly accurate in identifying sleep stage abnormalities when performed in a controlled sleep lab. However, accuracy depends on the quality of the recording and proper interpretation by a sleep specialist.